Thuốc kháng viêm không steroid (Non-steroidal anti-inflammatory drug: NSAID) là một trong những nhóm thuốc được kê đơn rộng rãi nhất trên thế giới, đặc biệt trong các bệnh lý cơ xương khớp, với hơn 100 triệu đơn thuốc được kê đơn hàng năm chỉ tính riêng ở Hoa Kỳ [1]. Ở Anh, ước tính mỗi năm có khoảng 50% bệnh nhân thoái hoá khớp được kê đơn NSAID uống, với chi phí lên đến 25,65 triệu bản Anh [2].
Vai trò của NSAID ở những bệnh nhân bị bệnh cơ xương khớp là không thể phủ nhận, tuy nhiên việc sử dụng NSAID có liên quan đến nhiều biến cố bất lợi, đặc biệt là các biến cố bất lợi trên tiêu hóa và tim mạch [3], [4], [5]. Chi phí để điều trị các biến cố liên quan đến việc sử dụng NSAID cũng rất đáng kể, ước tính khoảng 44,8-98 triệu bảng mỗi năm tại Anh [2].
NSAID là một trong những nguyên nhân hàng đầu gây ra các biến cố tiêu hoá nghiêm trọng như loét, xuất huyết tiêu hoá hoặc thủng dạ dày [6], [7]. Những biến cố bất lợi này được cho là dẫn đến việc nhập viện của hơn 100.000 người và 10.000 ca tử vong mỗi năm tại Hoa Kỳ [8], [9]. Bên cạnh đó, ngày càng có nhiều bằng chứng cho thấy NSAID có thể gây tăng huyết áp, làm tăng các biến cố bất lợi trên tim mạch như nhồi máu cơ tim hoặc đột quỵ ở cả những bệnh nhân có hoặc không có bệnh tim [10], [11], [12]. Các biến cố bất lợi của NSAID đặc biệt gia tăng ở những bệnh nhân có nhiều yếu tố nguy cơ [10], [13], [14], [15].
Các hướng dẫn điều trị hiện nay khuyến nghị, NSAID chỉ nên được kê đơn sau khi đã đánh giá các yếu tố nguy cơ của bệnh nhân, bao gồm tiền sử bệnh tiêu hoá và tim mạch, đồng thời theo dõi liên tục các yếu tố nguy cơ này trong suốt quá trình điều trị [7], [10]. Trong bất cứ trường hợp nào, việc cân bằng giữa lợi ích và nguy cơ sẽ là một cách tiếp cận hợp lý khi sử dụng NSAID [2], [16], [17].
Một số hướng dẫn điều trị khuyến nghị NSAID tại chỗ nên được xem xét trước NSAID uống do hiệu quả giảm đau và sự an toàn của dạng bào chế này, đặc biệt ở những bệnh nhân có nguy cơ cao [7], [18], [19], [20].
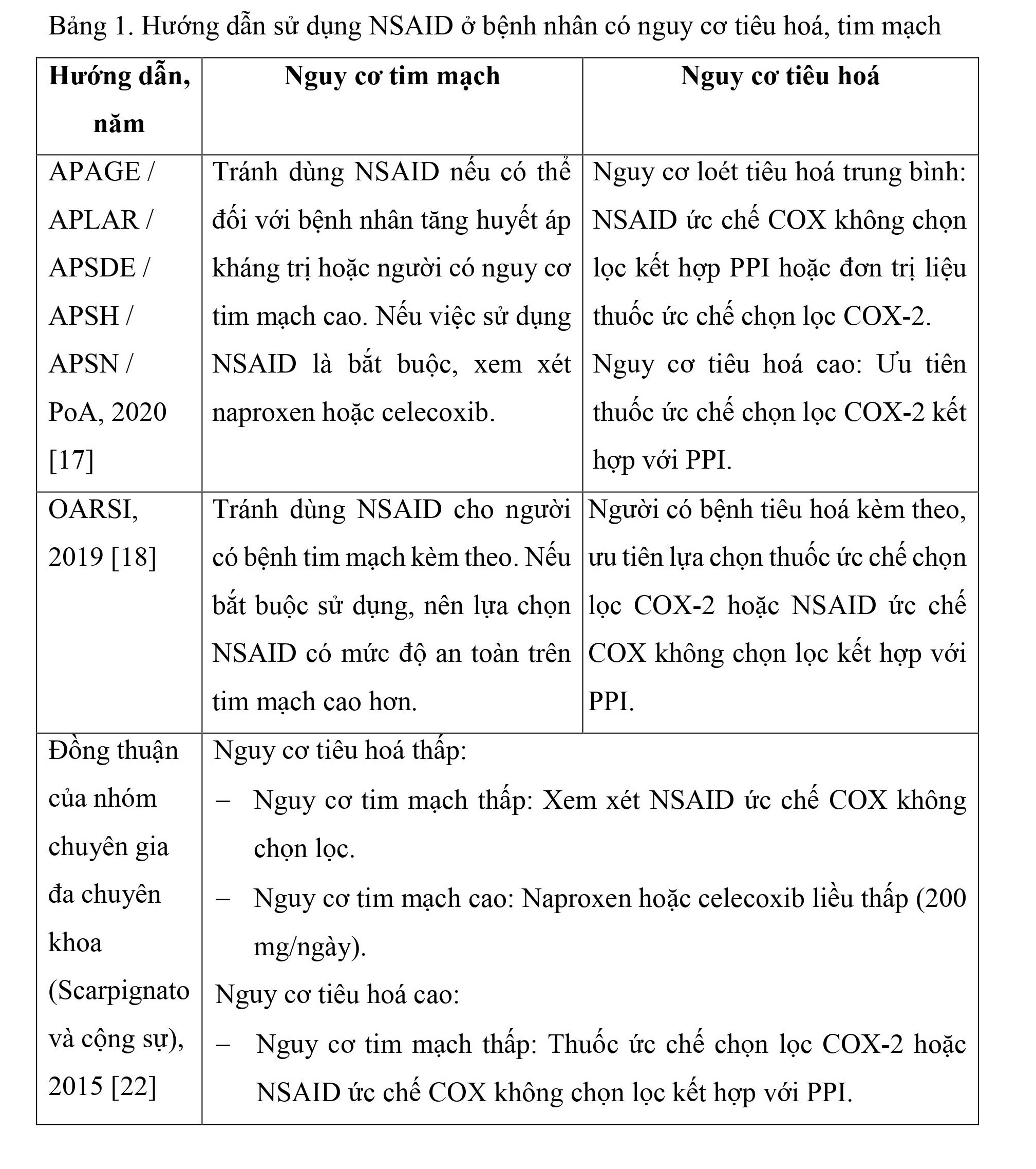
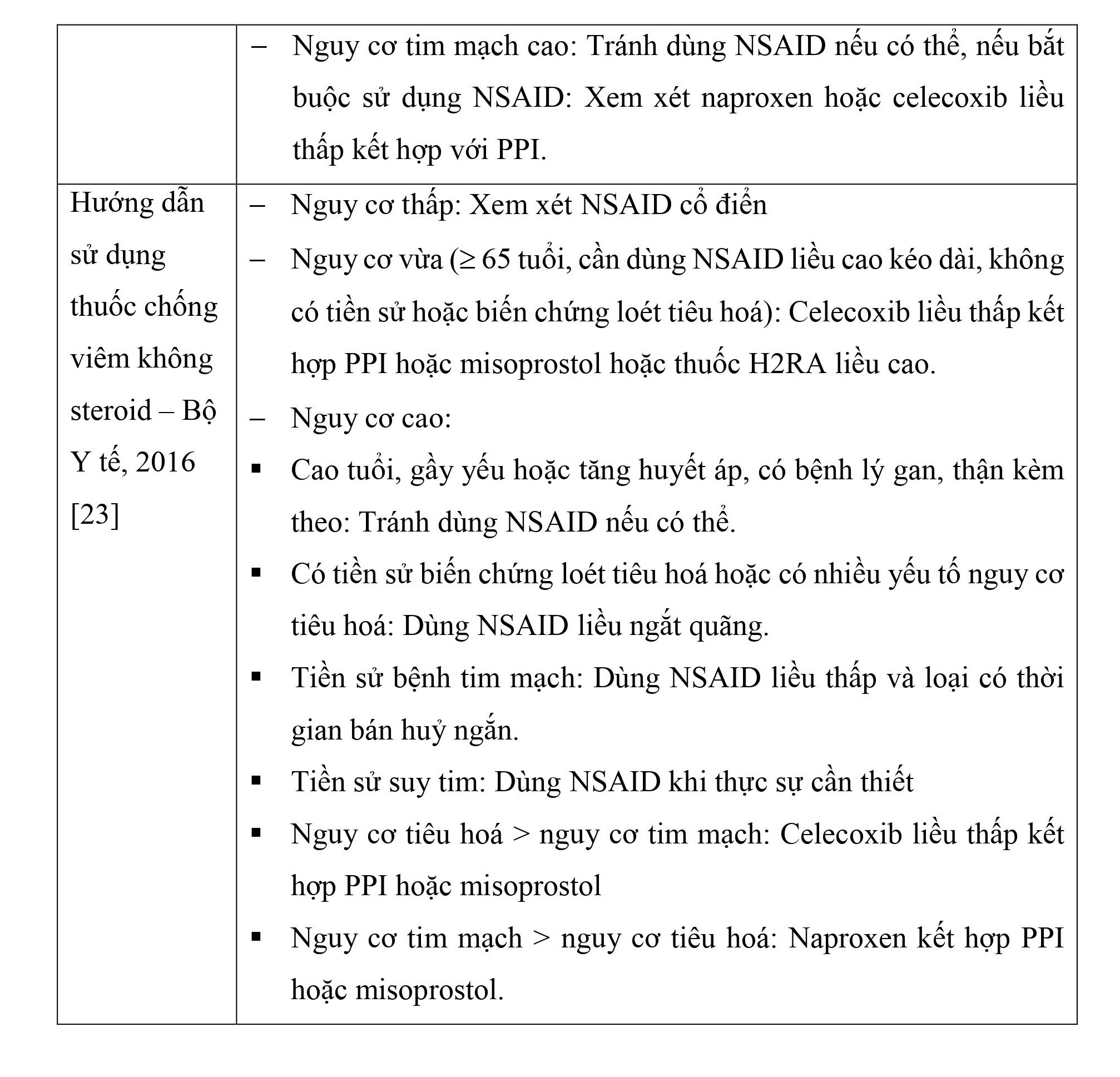
Khi NSAID uống được lựa chọn, các hướng dẫn điều trị hiện nay đều khuyến nghị rằng, nên sử dụng liều thấp nhất có hiệu quả, trong khoảng thời gian ngắn nhất có thể để giảm thiểu các biến cố bất lợi do NSAID gây ra [2], [16], [17], [19], [21]. Một số hướng dẫn sử dụng NSAID ở bệnh nhân có nguy cơ tiêu hoá và tim mạch được tóm tắt trong bảng 1.
TÀI LIỆU THAM KHẢO
[1] Walker Chris et al. (2018), "Cardiovascular safety of non-steroidal anti-inflammatory drugs revisited", Postgraduate medicine. 130 (1), pp. 55-71.
[2] Lau Chak Sing et al. (2015), "APLAR rheumatoid arthritis treatment recommendations", International Journal of Rheumatic Diseases. 18 (7), pp. 685-713.
[3] MacDonald Thomas M et al. (2016), "Randomized trial of switching from prescribed non-selective non-steroidal anti-inflammatory drugs to prescribed celecoxib: the Standard care vs. Celecoxib Outcome Trial (SCOT)", European heart journal. 38 (23), pp. 1843-1850.
[4] Mosleh Wassim et al. (2016), "Balancing cardiovascular and gastrointestinal risks in patients with osteoarthritis receiving nonsteroidal anti-inflammatory drugs", Pol Arch Med Wewn. 126 (1-2), pp. 68-75.
[5] Society Royal Pharmaceutical (2018), BNF 76 (British National Formulary) September 2018 - March 2019, Pharmaceutical Press, 1653: pp. 1095.
[6] Calatayud Sara et al. (2016), "Chemistry, pharmacodynamics, and pharmacokinetics of NSAIDs", NSAIDs and Aspirin, Springer, Switzerland, pp. 3-16.
[7] National Clinical Guideline Centre (2014), "National Institute for Health and Clinical Excellence: Guidance", Osteoarthritis: Care and Management in Adults, National Institute for Health and Care Excellence (UK), London, pp. 16-17.
[8] Bello Alfonso E et al. (2014), "Risk of upper gastrointestinal ulcers in patients with osteoarthritis receiving single-tablet ibuprofen/famotidine versus ibuprofen alone: pooled efficacy and safety analyses of two randomized, double-blind, comparison trials", Postgraduate medicine. 126 (4), pp. 82-91.
[9] Administration Food and Drug (2015), FDA Drug Safety Communication: FDA strengthens warning that non-aspirin nonsteroidal anti-inflammatory drugs (NSAIDs) can cause heart attacks or strokes, www.fda.gov/Drugs/DrugSafety/ucm451800.htm, ngày truy cập 05-03-2024.
[10] Fanelli Andrea et al. (2017), "Cardiovascular and cerebrovascular risk with nonsteroidal anti-inflammatory drugs and cyclooxygenase 2 inhibitors: latest evidence and clinical implications", Therapeutic advances in drug safety. 8 (6), pp. 173-182.
[11] Wong Sunny H et al. (2016), "Adverse Effects of NSAIDs in the Gastrointestinal Tract: Risk Factors of Gastrointestinal Toxicity with NSAIDs", NSAIDs and Aspirin, Springer, Switzerland, pp. 45-59.
[12] Administration Food and Drug (2015), FDA Drug Safety Communication: FDA strengthens warning that non-aspirin nonsteroidal anti-inflammatory drugs (NSAIDs) can cause heart attacks or strokes, www.fda.gov/Drugs/DrugSafety/ucm451800.htm, ngày truy cập 05-03-2024.
[13] Agency European Medicines (2015), Updated advice on use of high-dose ibuprofen, https://www.ema.europa.eu/en/news/updated-advice-use-high-dose-ibuprofen, ngày truy cập 05-03-2024.
[14] Walker Chris, Biasucci Luigi M. (2018), “Cardiovascular safety of non-steroidal anti-inflammatory drugs revisited”, Postgraduate medicine. 130 (1), pp. 55-71.
[15] Zeind Caroline S., Carvalho Michael G. (2018), "Rheumatic and musculoskeletal diseases", Applied therapeutics the clinical use of drugs, Philadelphia, pp. 887, 889.
[16] Practitioners The Royal Australian College of General (2018), Guideline for the management of knee and hip osteoarthritis, 2nd, The Royal Australian College of General Practitioners, East Melbourne, pp. 41.
[17] Szeto Cheuk-Chun et al. (2020), "Non-steroidal anti-inflammatory drug (NSAID) therapy in patients with hypertension, cardiovascular, renal or gastrointestinal comorbidities: joint APAGE/APLAR/APSDE/APSH/APSN/PoA recommendations", GUT. 69 (4), pp. 617-629.
[18] Bannuru Raveendhara R et al. (2019), "OARSI guidelines for the non-surgical management of knee, hip, and polyarticular osteoarthritis", Osteoarthritis and cartilage. 27 (11), pp. 1578-1589.
[19] Kloppenburg Margreet et al. (2019), "2018 update of the EULAR recommendations for the management of hand osteoarthritis", Annals of the rheumatic diseases. 78 (1), pp. 16-24.
[20] Kolasinski S. L. et al. (2020), "2019 American College of Rheumatology/Arthritis Foundation Guideline for the Management of Osteoarthritis of the Hand, Hip, and Knee", Arthritis Care and Research. 72 (2), pp. 149-162.
[21] National Guideline Centre (2018), "National Institute for Health and Care Excellence: Clinical Guidelines", Rheumatoid arthritis in adults: diagnosis and management, National Institute for Health and Care Excellence (UK), London, pp. 26.
[22] Scarpignato Carmelo et al. (2015), "Safe prescribing of non-steroidal anti-inflammatory drugs in patients with osteoarthritis an expert consensus addressing benefits as well as gastrointestinal and cardiovascular risks", BMC medicine. 13 (1), pp. 55.
[23] Bộ Y tế (2016), "Hướng dẫn sử dụng thuốc chống viêm không steroid", Hướng dẫn chẩn đoán và điều trị các bệnh cơ xương khớp, Nhà Xuất Bản Y học, Hà Nội, pp. 197-201.
ThS.DS Hà Xuân Tuấn - Khoa Dược
Bệnh Viện Đa Khoa Khu Vực Thủ Đức

